The Emperor of All Maladies : A Biography of Cancer (2010) - Siddhartha Mukherjee
Siddhartha Mukherjee (born 1970) is an Indian-born American physician, scientist and author. This book won the Pulitzer Prize for General Nonfiction and the Guardian Prize
Quelques notes sur ce #livre, qui est à mon avis plus une #histoire de la recherche sur le cancer qu’une “biographie du cancer”.
– p. 48. Le médecin romain Claude Galien (d’origine grecque), en 160, écrivait que le cancer provenait de l’accumulation d’une des quatre humeurs, la bile noire ; dépression et cancer étaient ainsi reliés de façon intrinsèque (cf. "Mars" de Fritz Zorn).
Only one other disease, replete with metaphors, would be attributed to an excess of this oily, viscous humor: depression. Indeed, melancholia, the medieval name for “depression,” would draw its name from the Greek melas, “black,” and khole, “bile.” Depression and cancer, the psychic and physical diseases of black bile, were thus intrinsically intertwined.) Galen proposed that cancer was “trapped” black bile—static bile unable to escape from a site and thus congealed into a matted mass.
– p. 86 ; 1910. Paul Ehrlich montre que la chimie industrielle va permettre de trouver des médicaments :
A gigantic factory, funded by Hoechst Chemical Works, was already being built to manufacture it for commercial use.
Ehrlich’s successes with Trypan Red and compound 606 (which he named Salvarsan, from the word salvation) proved that diseases were just pathological locks waiting to be picked by the right molecules. The line of potentially curable illnesses now stretched endlessly before him. Ehrlich called his drugs “magic bullets” — bullets for their capacity to kill and magic for their specificity. It was a phrase with an ancient, alchemic ring that would sound insistently through the future of oncology.
– p. 99 ; 1948, grâce à Sidney Farber et Mary Lasker (la mère de toutes les “ligues contre le cancer”), le cancer devient une cause « médiatique » :
The campaign against cancer, Farber learned, was much like a political campaign: it needed icons, mascots, images, slogans—the strategies of advertising as much as the tools of science. For any illness to rise to political prominence, it needed to be marketed, just as a political campaign needed marketing. A disease needed to be transformed politically before it could be transformed scientifically
– p. 119 ; l’aboutissement du projet Manhattan transforme la manière de penser la recherche ; le modèle de Vannevar Bush (donner la liberté aux chercheurs de se consacrer à la recherche fondamentale) semble subitement dépassé :
On August 7, 1945, the morning after the Hiroshima bombing, the New York Times gushed about the extraordinary success of the project: “University professors who are opposed to organizing, planning and directing research after the manner of industrial laboratories . . . have something to think about now. A most important piece of research was conducted on behalf of the Army in precisely the means adopted in industrial laboratories. End result: an invention was given to the world in three years, which it would have taken perhaps half-a-century to develop if we had to rely on prima-donna research scientists who work alone. . . . A problem was stated, it was solved by teamwork, by planning, by competent direction, and not by the mere desire to satisfy curiosity.”
The congratulatory tone of that editorial captured a general sentiment about science that had swept through the nation.
(Bien entendu c’est un leurre, car l’application technologique n’a pu fonctionner que sur une base scientifique fondamentale non dirigée.)
– p. 130 ; 1995 : l’invention des premiers essais cliniques en cancéro, avec l’implication des médecins cliniciens
As new drugs, combinations, and trials proliferated, [Gordon] Zubrod worried that institutions would be caught at cross-purposes, squabbling over patients and protocols when they should really be battling cancer. Burchenal in New York, Farber in Boston, James Holland at Roswell Park, and the two Emils at the NCI were all chomping at the bit to launch clinical trials. And since ALL was a rare disease, every patient was a precious resource for a leukemia trial. To avert conflicts, Zubrod proposed that a “consortium” of researchers be created to share patients, trials, data, and knowledge.
The proposal changed the field. “Zubrod’s cooperative group model galvanized cancer medicine,” Robert Mayer (who would later become the chair of one of these groups) recalls. “For the first time, an academic oncologist felt as if he had a community. The cancer doctor was not the outcast anymore, not the man who prescribed poisons from some underground chamber in the hospital.” The first group meeting, chaired by Farber, was a resounding success. The researchers agreed to proceed with a series of common trials, called protocols, as soon as possible.
Zubrod next set about organizing the process by which trials could be run. Cancer trials, he argued, had thus far been embarrassingly chaotic and disorganized. Oncologists needed to emulate the best trials in medicine.
– p. 135 ; sur l’expression « war on cancer », cette citation :
. . . But I do subscribe to the view that words have very powerful texts and subtexts. “War” has truly a unique status, “war” has a very special meaning. It means putting young men and women in situations where they might get killed or grievously wounded. It’s inappropriate to retain that metaphor for a scholarly activity in these times of actual war. The NIH is a community of scholars focused on generating knowledge to improve the public health. That’s a great activity. That’s not a war.
—Samuel Broder, NCI director
– p. 182 comment une maladie capture l’imagination en fonction des préoccupations de la société :
AIDS loomed so large on the 1980s in part because this was a generation inherently haunted by its sexuality and freedom; SARS set off a panic about global spread and contagion at a time when globalism and social contagion were issues simmering nervously in the West. Every era casts illness in its own image. Society, like the ultimate psychosomatic patient, matches its medical afflictions to its psychological crises; when a disease touches such a visceral chord, it is often because that chord is already resonating.
So it was with cancer. As the writer and philosopher Renata Salecl described it, “A radical change happened to the perception of the object of horror” in the 1970s, a progression from the external to the internal. In the 1950s, in the throes of the Cold War, Americans were preoccupied with the fear of annihilation from the outside: from bombs and warheads, from poisoned water reservoirs, communist armies, and invaders from outer space. The threat to society was perceived as external. Horror movies—the thermometers of anxiety in popular culture—featured alien invasions, parasitic occupations of the brain, and body snatching: It Came from Outer Space or The Man from Planet X.
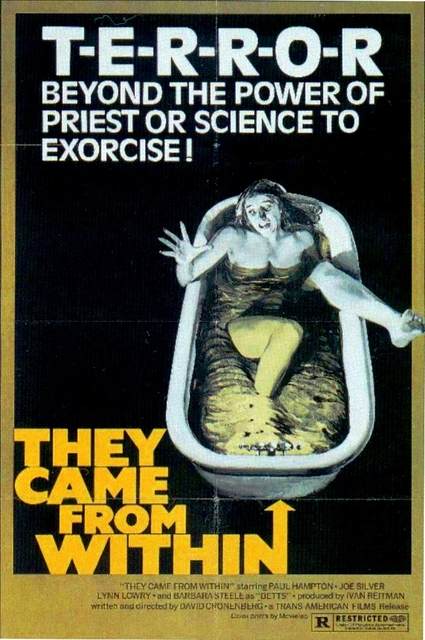
But by the early 1970s, the locus of anxiety—the “object of horror,” as Salecl describes it—had dramatically shifted from the outside to the inside. The rot, the horror—the biological decay and its concomitant spiritual decay—was now relocated within the corpus of society and, by extension, within the body of man. American society was still threatened, but this time, the threat came from inside. The names of horror films reflected the switch: The Exorcist; They Came from Within.
Cancer epitomized this internal horror.
– p. 198 ; à une période s’est développé ce qu’on appelait la « mastectomie radicale » de Halsted, une ablation non seulement du sein mais remontant le plus haut possible, jusqu’à la clavicule… l’idée qui avait amené à ce dogme était que, comme certaines patientes rechutaient ne guérissaient pas après une ablation, c’est qu’elle n’avait pas été suffisamment large ; aucune étude statistique n’avait démontré que cette boucherie apportait la moindre amélioration de la survie. En 1953, le chirurgien George Barney Crile se dit qu’il faut peut-être faire une analyse #statistique pour voir si réellement c’est efficace. Il se heurte alors au conservatisme de l’institution :
No breast cancer trial, for instance, could have proceeded without the explicit blessing and participation of larger-than-life surgeons such as Haagensen and Urban. Yet these surgeons, all enraptured intellectual descendants of Halsted, were the least likely to sponsor a trial that might dispute the theory that they had so passionately advocated for decades. When critics wondered whether Haagensen had been biased in his evaluation by selecting only his best cases, he challenged surgeons to replicate his astounding success using their own alternative methods: “Go thou and do likewise.”
Thus even Crile—a full forty years after Keynes’s discovery—couldn’t run a trial to dispute Halsted’s mastectomy. The hierarchical practice of medicine, its internal culture, its rituals of practice (“The Gospel[s] of the Surgical Profession,” as Crile mockingly called it), were ideally arranged to resist change and to perpetuate orthodoxy. Crile found himself pitted against his own department, against friends and colleagues. The very doctors that he would need to recruit to run such a trial were fervently, often viciously, opposed to it. “Power,” in the colloquial sense of the word, thus collided with “power” in the statistical sense. The surgeons who had so painstakingly created the world of radical surgery had absolutely no incentive to revolutionize it.
It took a Philadelphia surgeon named Bernard Fisher to cut through that knot of surgical tradition.
– p. 199 fin des années 1960 ; le #féminisme permet enfin pour la première fois au patient de s’ingérer dans la politique de santé :
In Texas, Jane Roe (a pseudonym) sued the state for blocking her ability to abort her fetus at a medical clinic—launching the Roe v. Wade case on abortion and highlighting the complex nexus between the state, medical authority, and women’s bodies. Political feminism, in short, was birthing medical feminism—and the fact that one of the most common and most disfiguring operations performed on women’s bodies had never been formally tested in a trial stood out as even more starkly disturbing to a new generation of women. “Refuse to submit to a radical mastectomy,” Crile exhorted his patients in 1973.
And refuse they did. Rachel Carson, the author of Silent Spring and a close friend of Crile’s, refused a radical mastectomy (in retrospect, she was right: her cancer had already spread to her bones and radical surgery would have been pointless). Betty Rollin and Rose Kushner also refused and soon joined Carson in challenging radical surgeons. Rollin and Kushner—both marvelous writers: provocative, down-to-earth, no-nonsense, witty—were particularly adept at challenging the bloated orthodoxy of surgery. They flooded newspapers and magazines with editorials and letters and appeared (often uninvited) at medical and surgical conferences, where they fearlessly heckled surgeons about their data and the fact that the radical mastectomy had never been put to a test.
(…)
“The clinician, no matter how venerable, must accept the fact that experience, voluminous as it might be, cannot be employed as a sensitive indicator of scientific validity,” [Bernard] Fisher wrote in an article. He was willing to have faith in divine wisdom, but not in Halsted as divine wisdom. “In God we trust,” he brusquely told a journalist. “All others [must] have data.”
(…)
Between 1891 and 1981, in the nearly one hundred years of the radical mastectomy, an estimated five hundred thousand women underwent the procedure to “extirpate” cancer.
– p. 204 ; l’arrivée du cisplatine, use molécule décrite en 1890, et testée par hasard sur le cancer en 1965 : "In 1973, the survival rate from metastatic testes cancer was less than 5 percent." Quelques années plus tard, les résultats sont miraculeux.
– p. 270 ; chapitre hallucinant sur les fabricants de #tabac ; le combat judiciaire est passionnant, avec notamment :
The tobacco industry had all but declared absolute victory: “Plaintiff attorneys can read the writing on the wall,” one report crowed, “they have no case.”
Edell, however, refused to read any writing on any walls. He acknowledged openly that Rose Cipollone was aware of the risks of smoking. Yes, she had read the warning labels on cigarettes and the numerous magazine articles cut out so painstakingly by Tony Cipollone. Yet, unable to harness her habit, she had remained addicted. Cipollone was far from innocent, Edell conceded. But what mattered was not how much Rose Cipollone knew about tobacco risks; what mattered was what cigarette makers knew, and how much of the cancer risk they had revealed to consumers such as Rose.
The argument took the tobacco companies by surprise. Edell’s insistence that he needed to know what cigarette makers knew about smoking risks allowed him to ask the courts for unprecedented access to the internal files of Philip Morris, Liggett, and Lorillard. Armed with powerful legal injunctions to investigate these private files, Edell unearthed a saga of epic perversity. Many of the cigarette makers had not only known about the cancer risks of tobacco and the potent addictive properties of nicotine, but had also actively tried to quash internal research that proved it. Document after document revealed frantic struggles within the industry to conceal risks, often leaving even its own employees feeling morally queasy.
– p. 275 ;
It is difficult for me to convey the range and depth of devastation that I witnessed in the cancer wards that could be directly attributed to cigarette smoking. (…) It remains an astonishing, disturbing fact that in America—a nation where nearly every new drug is subjected to rigorous scrutiny as a potential carcinogen, and even the bare hint of a substance’s link to cancer ignites a firestorm of public hysteria and media anxiety—one of the most potent and common carcinogens known to humans can be freely bought and sold at every corner store for a few dollars.
– p. 316, années 1980 ; l’arrivée du sida et de malades qui prennent en mains la connaissance scientifique et parlent sur un pied d’égalité avec les médecins
– p. 328, décembre 1999 : l’affaire Werner Bezwoda ; depuis les années 1980 la mode est à l’autogreffe de moelle osseuse. Ce chirurgien sud-africain, qui opère à Johannesburg, présente à chaque colloque des résultats fantastiques. L’industrie de transplantation engendrée par ces résultats engouffre 4 milliards de dollars. Mais des gens commencent à douter car leurs résultats ne sont pas si probants. Des enquêteurs sont envoyés pour vérifier — Bezwoda, qui n’opérait pratiquement que des femmes noires pauvres et illettrées, avait falsifié ses essais.
– p. 358, on croise Peter Duesberg, et ses recherches sur le Rous sarcoma virus (RSV). (Il deviendra plus tard l’inspirateur des négationnistes du lien entre VIH et sida.)
– p. 378, portrait de Thad Dryja, un collectionneur obsessionnel de tumeurs, qui va jusqu’à appeler les patients chez eux pour savoir s’ils ont d’autres membres de la famille touchés par le rétinoblastome, et n’hésite pas à prendre l’avion pour aller récupérer les tumeurs. Cela lui permettra de mettre en route toute la recherche sur la génétique du cancer.
– p. 388-389, une description minutieuse de la manière dont les mutations s’accumulent, conduisant progressivement au cancer. (“Let us begin with a normal cell…”)
– p. 418 ; l’histoire de l’herceptine chez Genentech, la recherche privée, les #brevets, le hiatus entre la recherche fondamentale et appliquée. Et là aussi l’arrivée des patients-militants, notamment Barbara Bradfield.
– p. 436 ; l’invention du Gleevec (Glivec) chez Ciba-Geigy (aujourd’hui Novartis), là encore, l’industriel ne voit pas l’intérêt de développer le médicament (les essais lui coûtant 100 M$), et le chercheur, Peter Drucker, doit se battre pour qu’il existe. On connaît la suite (hello l’Inde).
#cancer #recherche #santé #militer