This thread is long, and hard to read - not just because of the technical language, but because “it’s just a cold,” “the vaccine protects me,” and “at least our children are safe” are comforting fairy tales.
I wish they were true.
This virus is like measles and polio: a virus with long-term impact.
Even a “mild” case in a vaccinated individual can lead to long-term issues which cause a measurable uptick in all-cause mortality in the first 6 months, and get progressively worse with time.
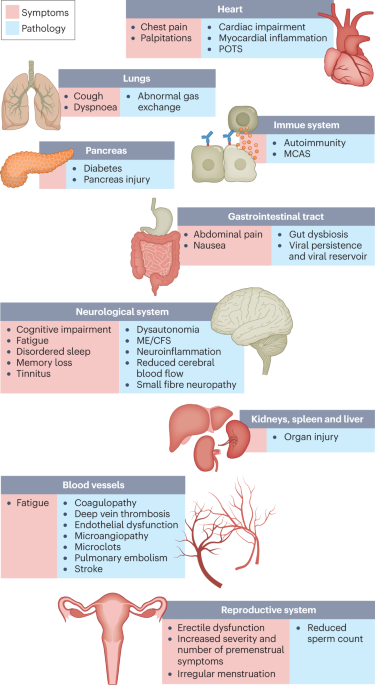
SARS-CoV-2 is a systemic disease which has multiple avenues to induce long-term impairment, attacking the brain, heart, lungs, blood, testes, colon, liver, and lymph nodes, causing persistent symptoms in more than half of patients by six months out.
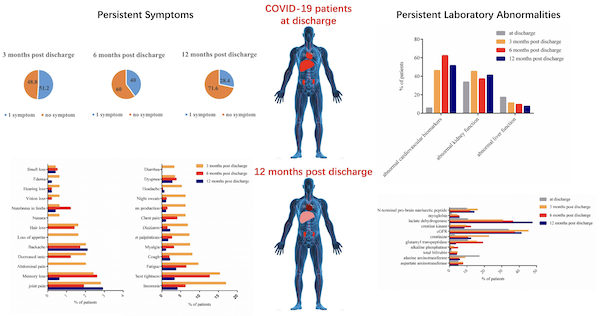
The CoVHORT study, limited to non-hospitalized patients in Arizona - “mild” cases - found a 68% prevalence of 1 or more Covid symptom after 30 days, rising to 77% after 60 days. (We will explore an explanation later).
▻https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0254347
To prevent panic, @CDCgov has been using the term “mild” to describe any case of COVID-19 which does not require hospitalization.
#LongCOVID, however, is anything but “mild”, as the replies to @ahandvanish’s thread make heartbreakingly clear.
▻https://twitter.com/ahandvanish/status/1423017721822949376
A University of Washington study found that 30% of Covid patients had reduced Health Related Quality of Life, with 8% of the patients limited in routine daily activities.
▻https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2776560
These patients are struggling with real physical issues.
This Yale study demonstrated reduced aerobic capacity, oxygen extraction. and ventilatory efficiency in “mild” COVID patients even after recovery from their acute infection.
▻https://journal.chestnet.org/article/S0012-3692(21)03635-7/abstract
It’s also a vascular disease. A Columbia study found “significantly altered lipid metabolism” during acute disease, which “suggests a significant impact of SARS-CoV-2 infection on red blood cell structural membrane homeostasis.”
▻https://pubs.acs.org/doi/full/10.1021/acs.jproteome.0c00606
Oregon Health & Science University found that “symptomatic or asymptomatic SARS-CoV-2 infection is associated with increased risk of [fatal] cardiovascular outcomes and has causal effect on all-cause mortality.”
▻https://www.medrxiv.org/content/10.1101/2021.12.27.21268448v1
Let’s review: SARS-CoV-2 causes an increase in mortality and reduced aerobic capacity even after asymptomatic cases, and remains in the body months after the initial infection.
No, it’s not “just a cold.”
But we’re just getting started. It gets worse. Way worse.
The virus appears to be able to cross the blood-brain barrier and cause significant neurological damage.
The ability of the spike protein to cross the blood-brain barrier was demonstrated in mice at the University of Washington.
▻https://pubmed.ncbi.nlm.nih.gov/33328624
A joint study by Stanford and Germany’s Saarland University found inflammation in the brain, and “show[ed] that peripheral T cells infiltrate the parenchyma.”
▻https://www.nature.com/articles/s41586-021-03710-0
For context, the parenchyma is the functional tissue of the brain - your neurons and glial cells. It isn’t normally where T cells are:
“In the brain of healthy individuals, T cells are only present sporadically in the parenchyma.”
▻https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6751344
The Stanford study also discovered microglia and astrocytes which displayed “features .. that have previously been reported in human neurodegenerative disease.”
Post-mortem neuropathology in Hamburg, Germany found “Infiltration by cytotoxic T lymphocytes .. in the brainstem and cerebellum, [with] meningeal cytotoxic T lymphocyte infiltration seen in 79% [of] patients.”
▻https://www.sciencedirect.com/science/article/pii/S1474442220303082#
An autopsy of a 14-month-old at Brazil’s Federal University of Rio de Janeiro found that “The brain exhibited severe atrophy and neuronal loss.”
▻https://www.thelancet.com/journals/lanam/article/PIIS2667-193X(21)00038-7/abstract
The UK Biobank COVID-19 re-imaging study compared before and after images of “mild” cases, and found “pronounced reduction in grey matter” and an “increase of diffusion indices, a marker of tissue damage” in specific regions of the brain.
▻https://www.medrxiv.org/content/10.1101/2021.06.11.21258690v3
That seems to explain why there is evidence of persistent cognitive deficits in people who have recovered from SARS-CoV2 infection in Great Britain.
▻https://www.thelancet.com/journals/eclinm/article/PIIS2589-5370(21)00324-2/fulltext
Also worrisome are syncytia, where an infected cell extrudes its own spike protein and takes over its neighbors, fusing together to create a large multi-nucleus cell.
Delta’s particular aptitude for this may partly explain its severity.
▻https://www.news-medical.net/news/20211006/SARS-CoV-2-emerging-variants-display-enhanced-syncytia-formation.aspx
And, yes, syncytia formation can happen in neurons. For our visual learners, here is video of syncytia and apoptosis (cell death) in a (bat) brain:
▻https://twitter.com/nytimes/status/1429604323047133185
Luckily, the University of Glasgow found that “Whilst Delta is optimised for fusion at the cell surface, Omicron .. achieves entry through endosomal fusion. This switch .. offers [an] explanation for [its] reduced syncytia formation.”
▻https://www.gla.ac.uk/media/Media_829360_smxx.pdf
If you’re interested in further understanding the host of neurological symptoms and the mechanisms underlying them, this Nature article is an excellent primer:
►https://www.nature.com/articles/d41586-021-01693-6
Let’s review: SARS-CoV-2 can cross the blood-brain barrier, and even “mild” or asymptomatic cases can cause loss of neurons and persistent cognitive defects?
That doesn’t sound “mild” to me; I like my brain.
But it keeps getting worse.
The brain isn’t the only organ affected: Testicular pathology has found evidence of “SARS-Cov-2 antigen in Leydig cells, Sertoli cells, spermatogonia, and fibroblasts” in post-morten examination.
▻https://onlinelibrary.wiley.com/doi/10.1111/andr.13073
A Duke pathology study in Singapore “detected SARS-CoV-2 .. in the colon, appendix, ileum, haemorrhoid, liver, gallbladder and lymph nodes .. suggesting widespread multiorgan involvement of the viral infection.”
▻https://gut.bmj.com/content/gutjnl/early/2021/06/13/gutjnl-2021-324280.full.pdf#page1
The same study found “evidence of residual virus in .. tissues during the convalescent phase, up to 6 months after recovery, in a non-postmortem setting,” suggesting that “a negative swab result might not necessarily indicate complete viral clearance from the body.”
It also causes microclots: “Fibrin(ogen) amyloid microclots and platelet hyperactivation [were] observed in [Long COVID] patients,” in this work by Stellenbosch University of South Africa, which also explored potential treatments.
▻https://www.researchsquare.com/article/rs-1205453/v1
Let’s review - SARS-CoV2 attacks our veins, blood, heart, brain, testes, colon, appendix, liver, gallbladder and lymph nodes?
No, it’s not “just a respiratory virus”.
Not even close.
There are also immunology implications:
Johns Hopkins’ @fitterhappierAJ found that “CD95-mediated [T cell] differentiation and death may be advancing T cells to greater effector acquisition, fewer numbers, and immune dysregulation.”
▻https://www.frontiersin.org/articles/10.3389/fimmu.2020.600405/full
This Chinese military study of the initial Wuhan outbreak concluded that “T cell counts are reduced significantly in COVID-19 patients, and the surviving T cells appear functionally exhausted.”
▻https://www.frontiersin.org/articles/10.3389/fimmu.2020.00827/full
The study authors went on to warn, “Non-ICU patients with total T cells counts lower than 800/μL may still require urgent intervention, even in the immediate absence of more severe symptoms due to a high risk for further deterioration in condition.”
Those warnings have since been proven by discovery of autoimmune features.
This study of 177 Los Angeles healthcare workers found that all had persistent self-attacking antibodies at least 6 months after infection, regardless of illness severity.
▻https://translational-medicine.biomedcentral.com/articles/10.1186/s12967-021-03184-8
In the words of T-cell immunologist Dr. Leonardi (@fitterhappierAJ)
▻https://twitter.com/fitterhappierAJ/status/1475227891034210314
This Kaiser Permanente S.California study found that, although natural immunity provided substantial protection against reinfection, “Hospitalization was more common at suspected reinfection (11.4%) than initial infection (5.4%).”
▻https://www.clinicalmicrobiologyandinfection.com/article/S1198-743X(21)00422-5/abstract
In fact, remember those cytokine storms? It turns out that even that even severe COVID-19 may not be a viral pneumonia, but an autoimmune attack of the lung.
▻https://twitter.com/DaveLeeERMD/status/1413816137570205697
Let’s review - it’s autoimmune: SARS-CoV2 convinces our body to attack itself.
That might explain why the Arizona study saw more symptoms after 60 days than at 30 days.
It also means “natural immunity” isn’t something to count on.
But if you’re counting on vaccination to feel safe, there’s even more bad news.
A study of Israel healthcare workers found that “Most breakthrough cases were mild or asymptomatic, although 19% had persistent symptoms (>6 weeks).”
►https://www.nejm.org/doi/full/10.1056/NEJMoa2109072
Perhaps the most terrifying study is from Oxford University, which examined the effects of vaccination on long COVID symptoms, because not only did it find that vaccination does not protect against Long Covid, but that Long Covid symptoms become more likely over time:
In the words of the study authors, “vaccination does not appear to be protective against .. long-COVID features, arrhythmia, joint pain, type 2 diabetes, liver disease, sleep disorders, and mood and anxiety disorders."
▻https://www.medrxiv.org/content/10.1101/2021.10.26.21265508v3
“The narrow confidence intervals rule out the possibility that these negative findings are merely a result of lack of statistical power. The inclusion of death in a composite endpoint with these outcomes rules out survivorship bias as an explanation.”
That finding contradicts the findings from the UK Zoe app study, which found that “the odds of having symptoms for 28 days or more after post-vaccination infection were approximately halved by having two vaccine doses.”
▻https://www.thelancet.com/journals/laninf/article/PIIS1473-3099(21)00460-6/fulltext
However, the structural limitations of the Zoe study - discussed in detail by @dgurdasani1 in the linked thread - may explain why it is particularly susceptible to bias against detecting a progressive degenerative condition.
▻https://twitter.com/dgurdasani1/status/1422802883632893952
Let’s review: we’ve now shown that vaccination appears to offer no protection against the long-term autoimmune effects of COVID - which we know causes T-cells to attack the lungs, and can cause T-cells to enter the brain.
Why are we letting this run wild?!
You may think, at least our children are safe.
They are not.
The CDC is tracking incidence of a life-threatening multisystem inflammatory syndrome in children following an acute COVID-19 infection, with 5,973 cases as of November 30, 2021.
▻https://covid.cdc.gov/covid-data-tracker/#mis-national-surveillance
Children also suffer from Long Covid.
“More than half [of pediatric patients] reported at least one persisting symptom even 120 days [after] COVID-19, with 42.6% impaired by these symptoms during daily activities.”
►https://www.medrxiv.org/content/10.1101/2021.01.23.21250375v1
Focusing exclusively on pediatric deaths is vastly underselling the danger to children.
Anybody telling you that SARS-CoV-2 is “just a cold” or “safe for children” is lying to you. They are ignoring the massive body of research that indicates that it is anything but.
Since our vaccines don’t stop transmission, and don’t appear to stop long-term illness, a “vaccination only” strategy is not going to be sufficient to prevent mass disability.
This isn’t something we want to expose our kids to.
Let’s review: even for children and vaccinated people, a “mild” case of COVID causes symptoms that point to long-term autoimmune issues, potentially causing our own body to attack our brains, hearts, and lungs.
Scared? Good.
Now we’re ready to get to work.
“This is the virus most Americans don’t know. We were born into a world where a virus was a thing you got over in a few weeks.” — @sgeekfemale, to whom I owe a “thank you” for her editing assistance on this thread.
The viruses they know in Kolkota, Kinshasa, and Wuhan are different: dangerous, lethal beasts.
Since 2020, the field has been leveled. Willing or no, we’ve rejoined the rest of the world. We are, all of us, vulnerable in the face of an unfamiliar threat.
The first step is acknowledging the threat.
That means acknowledging that our response has been woefully inadequate, and that is going to be uncomfortable.
The thought that we could have prevented this, but didn’t, will feel unconscionable to some.
The knowledge that we could start preventing this today, but haven’t, is unconscionable to me.
▻https://twitter.com/IanRicksecker/status/1426584062827712512
It’s time to quit pretending “it’s just a cold,” or that there is some magical law of viruses that will make it evolve to an acceptable level.
There’s no such law of evolution, just wishful thinking, easily disproven by:
Ebola. Smallpox. Marburg. Polio. Malaria.
There are things we can do to reduce our individual risk, immediately.
That starts with wearing a good mask - an N95 or better - and choosing to avoid things like indoor dining and capacity-crowd stadiums.
▻https://twitter.com/LazarusLong13/status/1440398111445188618
This isn’t a choice of “individual freedom” vs “public health”. It isn’t “authoritarian” to ask people to change their behavior in order to save lives.
▻https://www.thehastingscenter.org/individual-freedom-or-public-health-a-false-choice-in-the-covid-e
As Arnold @Schwarzenegger argued so convincingly in @TheAtlantic, it is our patriotic duty:
“Generations of Americans made incredible sacrifices, and we’re going to throw fits about putting a mask over our mouth and nose?”
▻https://www.theatlantic.com/ideas/archive/2021/08/schwarzenegger-schmuck-mask-vaccines/619746
“Those who would sacrifice essential liberty for a little bit of temporary security deserve neither!”
What is the essential liberty here?
It is the liberty to be able to breathe clean air, to live our lives without infecting our families and risking disability.
To get there, we need to listen to our epidemiologists and public health experts - the ones who have been trying to tell us this since the beginning:
▻https://twitter.com/EpiEllie/status/1444088804961304581
It is time — long past time — to give up on the lazy fantasy that we can let it become “endemic” and “uncontrolled” because it inconveniences us, because it is killing our political opponents, or because the virus will magically evolve to some “mild” state.
It is time — long past time — to begin controlling this virus.
It’s possible: Japan, New Zealand, and South Korea have done it.
It saves lives:
It’s even good for the economy:
“Globally, economic contraction and growth closely mirror increases and decreases in COVID-19 cases... Public health strategies that reduce SARS-CoV-2 transmission also safeguard the economy.”
▻https://bmcinfectdis.biomedcentral.com/articles/10.1186/s12879-021-06357-4
It’s time.






















































{kind=link}